
Schedule Consultation
Advanced Cancer Treatment Highlights
- If your cancer is inoperable, contact us for an online consultation to explore advanced, minimally invasive, and robotic treatments for the best success rates.
- Our innovative, stitchless treatments allow patients to be discharged within 2-3 days and quickly resume their daily activities.
- We offer effective cancer treatment without the need for painful surgery or chemotherapy.
- These cutting-edge therapies are often exclusive to our hospital and are offered at competitive prices.
Understanding Pancreatic Cancer
Pancreatic cancer is a severe disease affecting the pancreas, a crucial organ for digestion and blood sugar regulation. Early detection and understanding the disease are essential for effective treatment.
Tailored Treatment for Pancreatic Cancer Stages
Pancreatic cancer varies in stages, and effective treatment depends on accurately assessing the stage of the cancer. Treatment approaches vary based on the extent of the disease and the patient’s overall health.
Early-Stage Pancreatic Cancer
Early detection is key to successful treatment. For patients with localized tumors, treatment options may include:
- Surgery: Surgical removal of the tumor (pancreatectomy).
- Chemotherapy: Medications to shrink tumors before surgery or as an adjuvant therapy.
These treatments aim to remove or shrink the tumor while preserving pancreatic function.
Advanced-Stage Pancreatic Cancer
Advanced-stage pancreatic cancer requires advanced therapies. Our hospital provides options including:
What is Cryosurgical Ablation (CSA) for Pancreatic Cancer?
Cryosurgical Ablation (CSA) is a cutting-edge procedure that destroys Pancreatic tumors using freezing and thawing cycles. While it’s highly effective, expertise in India is currently limited.
- Minimally Invasive: CSA requires only a small incision, leading to reduced recovery time and post-operative discomfort.
- Preservation of Healthy Tissue: It’s highly precise, ensuring that surrounding healthy tissue is not damaged.
- Repeatable: Can be repeated in cases of recurrent tumors, providing a versatile treatment option.
- Reduced Side Effects: Patients typically experience fewer side effects compared to other treatment methods.

What are Seed Knife Therapy (Brachytherapy) for Pancreatic Cancer?
Seed Knife Therapy, also known as Brachytherapy, involves implanting seeds that emit targeted radiation to destroy cancer cells. It’s a minimally invasive procedure with a quicker recovery time.
- Targeted Radiation: Precisely targets cancer cells, minimizing damage to healthy tissue.
- Minimally Invasive: Requires a small incision, leading to faster recovery.
Can Seed Knife Therapy provide a cure for Pancreatic cancer?
What is Percutaneous Ablation (Radiofrequency Ablation – RFA) for Pancreatic Cancer?
Percutaneous Ablation uses heat to effectively target and destroy tumors. It is minimally invasive, with reduced recovery time and post-operative discomfort.
- Effective in Destroying Cancer Cells: Uses heat to effectively target and destroy tumors.
Is Percutaneous Ablation a suitable treatment option for Pancreatic cancer?
What is Combined Immunotherapy for Pancreatic Cancer?
Combined Immunotherapy boosts the body’s natural immune functions against cancer cells. It has shown promising results when used in combination with other treatments like cryosurgery.
- Enhanced Immune Response: Strengthens the body’s ability to fight cancer cells.
- Potential Synergy with Other Treatments: Can complement existing therapies.
What are Targeted Therapies for Pancreatic Cancer?
Targeted Therapies refer to medications that specifically target cancer cells, inhibiting their growth.
- Precision Treatment: Targets cancer cells directly, minimizing damage to healthy cells.
- Reduced Side Effects: Patients often experience fewer side effects compared to traditional chemotherapy.
How effective is Transarterial chemo-injection in Pancreatic cancer treatment?
Transarterial chemo-injection is a targeted chemotherapy approach where medicine is deoraled directly to the cancerous area through the artery supplying blood. This leads to a significant increase in drug concentration within the cancer cells over a short period. While the high drug density may not be sustained, it offers fewer side effects compared to systemic chemotherapy
- Deorals chemo directly to cancerous area via artery
- Rapidly increases drug concentration in cancer cells
- Offers fewer side effects than systemic chemotherapy
What is Cancer Microvessel Intervention (CMI) ? and how it helps in curing Pancreatic Cancer?
Cancer Microvessel Intervention (CMI) involves combining different chemo medicines into fine-grain particles and distributing them inside the artery supplying the target cancer. These particles stay within the tumor tissue, maintaining high density for an extended period. This method capitalizes on the unique properties of cancer capillary endothelial cells, allowing the chemo particles to selectively constrict micro-capillaries and block blood flow, effectively trapping the medicine in the tumor. As a result, less chemo medicine is needed, reducing side effects on the body compared to systemic chemotherapy.
- Combines chemo into fine particles for targeted deoraly
- Maintains high drug density in tumor tissue for extended periods
- Selectively constricts cancer micro-capillaries, blocking blood flow
- Requires less chemo medicine, reducing overall side effects compared to systemic chemotherapy
Learn more about Cancer Microvessel Intervention (CMI).
Nano Knife Robotics Therapy
Learn more about Nano Knife (Irreversible Electroporation).
Our experts will assess your specific condition and recommend the most suitable treatment plan for advanced-stage pancreatic cancer.
Advanced-Stage, Inoperable pancreatic Cancer: Exploring Treatment Options
Some innovative therapies for advanced-stage or last stage pancreatic cancer:
Advanced Minimally Invasive Treatments:
If your cancer is in its last stage or deemed inoperable, consider Cryosurgery, NanoKnife IRE, or Brachytherapy. Cryosurgery and NanoKnife IRE are cutting-edge, minimally invasive treatments suitable for both localized and metastatic cancers. These procedures fall under the category of Robotic treatments, offering a one-time stitch-less approach.

Brachytherapy: Latest in Radiotherapy:
For those seeking the latest form of radiotherapy, Brachytherapy provides an effective solution. This procedure, based on Nano technology, involves Radioactive Seeds Implants through a minimally invasive process. It can be completed in a single day and is applicable for various cancers, including bone, prostate, pancreatic, lymph nodal metastases, gall-bladder, and sarcoma.

Microvascular Interventional Localised (Intra-arterial) Chemotherapy:
If you’re in search of the latest and most effective chemotherapy with minimal side-effects, consider Microvascular Interventional Localised (Intra-arterial) chemotherapy. Unlike systemic chemotherapy, this treatment targets the specific organ affected by cancer, sparing the rest of the body’s immune system. It is remarkably well-tolerated and six times more effective than traditional whole-body chemotherapy.
Patients with advanced-stage pancreatic cancer receive specialized care and advanced therapies:
- Biological Therapy: Medications targeting the biological processes that promote cancer growth.
- Precision Medicine: Treatment based on the specific genetic makeup of the cancer.
These advanced therapies aim to improve both the quality of life and treatment outcomes for advanced-stage pancreatic cancer patients.
Specialized Pancreatic Cancer Treatments
Additional treatment options for pancreatic cancer include:
- Whipple Procedure: A complex surgery to remove the head of the pancreas and surrounding tissues.
- Targeted Drug Therapies: Medications that target specific genetic mutations in cancer cells.
Our hospital offers a range of specialized treatments to address various aspects of pancreatic cancer care.
Best Hospital for Pancreatic Cancer Treatment in India
Choose our hospital for pancreatic cancer treatment for several reasons, including experienced professionals, advanced treatments, proven success, patient-centric care, and cost-effective options.
Our mission is to offer hope, healing, and support throughout your treatment journey. With our expertise in pancreatic cancer treatment in India, we are committed to enhancing your quality of life and providing the best possible outcomes.
Treatment Abroad vs. Indian Options
Consider treatment options in India for pancreatic cancer, which often provide high-quality care at a fraction of the cost compared to treatment abroad. We offer personalized and advanced therapies right here in India, making it convenient and cost-effective.
Our Hospital: Your Destination for Pancreatic Cancer Care
Our hospital is a trusted name in pancreatic cancer treatment in India. With state-of-the-art facilities and a dedicated team of professionals, we prioritize patient well-being and successful outcomes. Our expertise ensures that you receive the best care possible.
Why Choose Us for Pancreatic Cancer Treatment
Patients choose our hospital for pancreatic cancer treatment for several reasons:
- Experienced medical professionals specializing in pancreatic cancer.
- Advanced treatment approaches, including innovative therapies.
- Proven success in improving patient outcomes.
- Patient-centric care focused on comfort and well-being.
- Cost-effective treatments without compromising quality.
We are dedicated to providing the highest standard of care and support throughout your journey to recovery from pancreatic cancer.
Unique Features of Our Hospital
- Advanced Technology: We utilize state-of-the-art medical equipment and technology to provide cutting-edge treatments.
- Personalized Care: Each patient receives a customized treatment plan tailored to their specific condition.
- Experienced Specialists: Our team includes highly skilled and experienced medical professionals specializing in pancreatic cancer.
- Research and Innovation: Our hospital is dedicated to ongoing research and innovation in pancreatic cancer treatment.
- Global Network: We collaborate with renowned medical institutions worldwide to stay at the forefront of pancreatic cancer care.
These unique features set our hospital apart and ensure the best possible care for our patients.
What is the success rate for Pancreatic cancer treatment in India at fuda cancer hospital?
Here are some key statistics about our hospital’s pancreatic cancer treatment:
- 192 Number of pancreatic cancer patients treated annually.
- 65% Success rates in various stages of pancreatic cancer.
- Average recovery time for patients is 2 months.
- 7 Number of specialized medical professionals on our team.
These statistics reflect our commitment to providing high-quality care and improving patient outcomes.
Get in Touch with Our Experts
If you have questions about pancreatic cancer treatment or would like to schedule a consultation with our experts, please don’t hesitate to contact us. We are here to provide you with the information and support you need for your journey to healing and recovery.Contact Us
What are the primary functions of the pancreas?
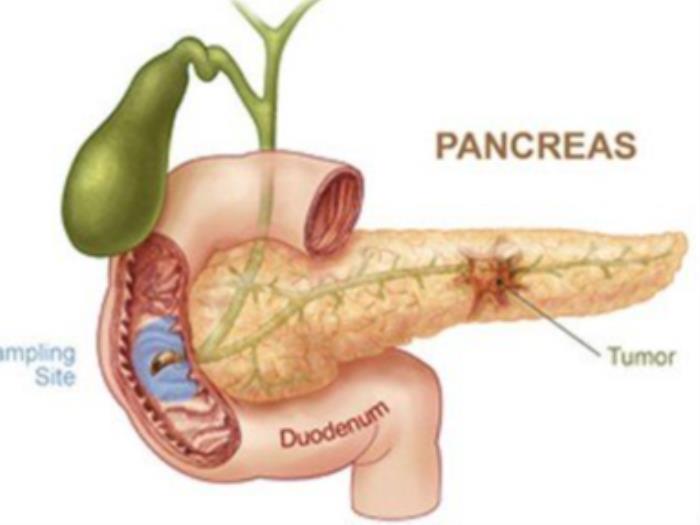
The pancreas is an organ located in the abdomen, behind the stomach. It has two main functions:
- Endocrine Function: The pancreas produces hormones like insulin and glucagon, which regulate blood sugar levels. Insulin lowers blood sugar, while glucagon raises it.
- Exocrine Function: The pancreas secretes enzymes into the small intestine to help break down food during digestion. These enzymes aid in the digestion of carbohydrates, proteins, and fats.
What is pancreatic cancer and its treatment in India?
Pancreatic cancer is a type of cancer that originates in the cells of the pancreas. In India, treatment options for pancreatic cancer depend on various factors, including the stage of cancer, the patient’s overall health, and the location of the tumor. Common treatments may include:
- Surgery: This involves removing part or all of the pancreas.
- Chemotherapy: Medications are used to kill cancer cells or stop their growth.
- Radiation Therapy: High-energy rays are used to target and kill cancer cells.
- Targeted Therapy: Specific drugs target the abnormalities in cancer cells.
Why does pancreatic cancer develop, and what are the treatment options in India?
Pancreatic cancer can develop due to a combination of genetic and environmental factors. Risk factors include smoking, obesity, family history, and certain genetic mutations. In India, treatment options include surgery, chemotherapy, radiation therapy, and targeted therapies. The choice of treatment depends on the stage and location of the cancer.
What are the causes of pancreatic cancer, and how is it treated in India?
The causes of pancreatic cancer are multifaceted. They may include genetic mutations, smoking, obesity, chronic pancreatitis, and family history. In India, treatment involves a comprehensive approach. Surgery, chemotherapy, and radiation therapy are common methods used to combat pancreatic cancer. Treatment plans are tailored to each individual’s specific condition.
What is the first sign of pancreatic cancer, and how is it addressed in India?
The first sign of pancreatic cancer can vary, but common symptoms include jaundice (yellowing of the skin and eyes), abdominal pain, unexplained weight loss, and changes in stool color. In India, prompt medical evaluation, including imaging tests like CT scans and MRIs, is crucial for early diagnosis. A specialized medical team will then develop a treatment plan tailored to the individual’s needs.
What methods can be used for self-detection of pancreatic cancer in India?
Self-detection of pancreatic cancer is challenging, as it often lacks early, specific symptoms. However, individuals should be aware of any persistent symptoms like abdominal pain, jaundice, unexplained weight loss, and changes in stool color. If these symptoms occur, seeking prompt medical attention in India is crucial for early diagnosis and treatment.
What are the risk factors for pancreatic cancer in India?
In India, risk factors for pancreatic cancer may include smoking, obesity, family history of the disease, chronic pancreatitis, and certain genetic mutations. Understanding these risk factors can help individuals take preventive measures and seek early medical intervention if needed.
What is the typical life expectancy after a diagnosis of pancreatic cancer in India?
The typical life expectancy after a diagnosis of pancreatic cancer in India can vary widely depending on the stage of cancer, overall health of the individual, and the chosen treatment approach. It’s important to discuss prognosis and treatment options with a healthcare team in India for personalized information.
What preventive measures can be taken against pancreatic cancer in India?
While it’s not always possible to prevent pancreatic cancer, there are some measures individuals can take in India to lower their risk:
- Quit smoking, as tobacco use is a major risk factor.
- Maintain a healthy weight through a balanced diet and regular exercise.
- Limit alcohol consumption, as excessive drinking is associated with an increased risk.
- Eat a diet rich in fruits, vegetables, and whole grains, and low in red and processed meats.
- Manage diabetes and chronic pancreatitis, as these conditions may increase the risk of pancreatic cancer.
- Consider genetic counseling if there’s a family history of pancreatic cancer or certain genetic mutations.
What are the different types of pancreatic cancer and their treatments in India?
Pancreatic cancer can be broadly classified into two main types: exocrine tumors and endocrine tumors.
Exocrine Tumors: These are the most common type and include adenocarcinomas. Treatment options in India may involve surgery, chemotherapy, radiation therapy, and targeted therapy.
Endocrine Tumors: Also known as neuroendocrine tumors, these are less common. Treatment may involve surgery, medications, and occasionally targeted therapy.
What are the different stages of pancreatic cancer and their management in India?
Pancreatic cancer is staged from I to IV based on the extent of the tumor’s spread. In India, management may involve:
- Stage I and II: Surgery to remove the tumor, followed by chemotherapy or radiation therapy.
- Stage III: A combination of chemotherapy and radiation therapy, followed by surgery if possible.
- Stage IV: Chemotherapy, targeted therapy, and palliative care to manage symptoms and improve quality of life.
What are the major tests to identify pancreatic cancer in India?
In India, diagnosing pancreatic cancer typically involves a combination of the following tests:
- Imaging tests like CT scans, MRIs, and ultrasounds to visualize the pancreas and surrounding areas.
- Endoscopic tests like endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP) for detailed imaging and biopsies.
- Blood tests to measure levels of certain markers associated with pancreatic cancer.
What are the potential side effects of advanced stage pancreatic cancer treatment in India?
Treatment for advanced-stage pancreatic cancer in India can have various side effects, including:
- Nausea and vomiting
- Fatigue
- Loss of appetite
- Weight loss
- Pain
- Changes in digestion
- Emotional and psychological effects
Are there experimental or emerging treatments for last-stage pancreatic cancer in India?
Yes, in India, there may be clinical trials and experimental treatments available for last-stage pancreatic cancer. These may include targeted therapies, immunotherapies, and other innovative approaches. It’s important to consult with a healthcare team to explore all available options.
How does nutrition and diet play a role in pancreatic cancer treatment in India?
Nutrition and diet are crucial aspects of pancreatic cancer treatment in India. A balanced diet helps maintain strength, supports the immune system, and aids in recovery. Recommendations may include:
- Consuming high-calorie, high-protein foods to prevent weight loss.
- Focusing on nutrient-dense foods like fruits, vegetables, and whole grains.
- Avoiding fatty, spicy, or hard-to-digest foods, which can exacerbate digestive symptoms.
- Working with a registered dietitian to create a personalized nutrition plan.
What support services are available for individuals undergoing pancreatic cancer treatment in India?
In India, individuals undergoing pancreatic cancer treatment have access to various support services:
- Oncology nurses and navigators who provide guidance and support throughout treatment.
- Palliative care teams to manage symptoms and improve quality of life.
- Support groups for emotional and psychological well-being.
- Access to social workers, counselors, and holistic healthcare providers.
Can complementary or alternative therapies be used alongside conventional treatment for pancreatic cancer in India?
Complementary or alternative therapies may be considered as part of a holistic approach to pancreatic cancer treatment in India. These therapies can include acupuncture, meditation, yoga, and dietary supplements. It’s important to discuss these options with the healthcare team to ensure they align with the overall treatment plan.
Is a biopsy needed for the treatment of pancreatic cancer in India?
Yes, a biopsy is a crucial step in confirming the diagnosis of pancreatic cancer in India. It involves the removal of a small sample of tissue for examination. This helps determine the type of cancer and informs the treatment plan.
Is pancreatic cancer curable, and what are the treatment options in India?
Pancreatic cancer can be challenging to cure, especially in advanced stages. However, early diagnosis and timely treatment in India can improve outcomes. Treatment options may include surgery, chemotherapy, radiation therapy, and targeted therapy, tailored to the individual’s condition.
Is it possible to be completely cured of pancreatic cancer in India?
Complete cure of pancreatic cancer depends on several factors, including the stage of cancer at diagnosis and the individual’s overall health. In some cases, especially in early stages, complete cure is possible with aggressive treatment. However, it’s important to discuss prognosis and treatment options with a healthcare team in India.
What are the common approaches of doctors to treat different stages of pancreatic cancer in India?
In India, doctors employ various approaches to treat different stages of pancreatic cancer:
- For early stages, surgery to remove the tumor is often the primary approach.
- Chemotherapy and radiation therapy may be used before or after surgery to shrink tumors and prevent recurrence.
- In advanced stages, a combination of chemotherapy, targeted therapy, and palliative care is typically employed.
Which is the best treatment for pancreatic cancer in India?
The best treatment for pancreatic cancer in India depends on various factors including the stage and location of the cancer, the patient’s overall health, and the expertise of the medical team. Common treatments may include surgery, chemotherapy, radiation therapy, and targeted therapy. A personalized treatment plan is determined after thorough evaluation by the healthcare team.
When should you go see a pancreatic cancer specialist doctor in India?
If you have any symptoms or risk factors associated with pancreatic cancer, it’s important to consult a specialist doctor in India promptly. Early diagnosis and treatment can significantly impact outcomes. Symptoms may include abdominal pain, jaundice, unexplained weight loss, and changes in stool color.
When is the optimal time to consult a specialist for pancreatic cancer in India?
The optimal time to consult a specialist for pancreatic cancer in India is as soon as you experience symptoms or if you have risk factors associated with the disease. Early diagnosis allows for timely intervention and potentially more effective treatment options.
How to choose the best oncologist for your pancreatic cancer treatment in India?
Choosing the best oncologist for pancreatic cancer treatment in India involves several considerations:
- Look for oncologists with expertise and experience in treating pancreatic cancer.
- Consider seeking referrals from trusted healthcare professionals or support groups.
- Research the oncologist’s credentials, affiliations, and patient reviews.
- Ensure the oncologist practices at a reputable healthcare institution with advanced facilities.
How to choose the best pancreatic cancer hospital in India?
Choosing the best pancreatic cancer hospital in India is a crucial decision. Consider the following factors:
- Look for hospitals with specialized oncology departments and experienced multidisciplinary teams.
- Research the hospital’s track record in treating pancreatic cancer and patient outcomes.
- Consider the availability of advanced diagnostic and treatment technologies.
- Ensure the hospital offers comprehensive support services for cancer patients.
Which country is best for pancreatic cancer treatment, and what are the options in India?
India is emerging as a hub for high-quality pancreatic cancer treatment. The country offers advanced medical facilities, skilled healthcare professionals, and a range of treatment options. Leading hospitals and cancer centers in cities like Mumbai, Delhi, and Bangalore provide world-class care for pancreatic cancer patients.
Who are the best doctors for pancreatic cancer treatment in India?
India is home to many accomplished oncologists specializing in pancreatic cancer treatment. Some renowned doctors in the field include Dr. Shailesh Shrikhande, Dr. Sudeep Gupta, and Dr. Rakesh Jalali, among others. It’s recommended to research and consult with healthcare professionals to find the best fit for your specific case.
What is the cost of pancreatic cancer treatment in India?
The cost of pancreatic cancer treatment in India can vary widely depending on factors such as the stage of cancer, the chosen treatment approach, the hospital, and additional services required. On average, the expenses may range from INR 5,00,000 to 20,00,000 or more. It’s crucial to consult with healthcare providers and financial advisors for personalized cost estimates.
Which is the best hospital for pancreatic cancer in India?
Several hospitals in India are renowned for their expertise in pancreatic cancer treatment. Some of the top hospitals include Tata Memorial Hospital in Mumbai, All India Institute of Medical Sciences (AIIMS) in Delhi, and Apollo Hospitals in various cities. It’s essential to research and consider factors like specialization, infrastructure, and patient outcomes when choosing a hospital.
Leading Pancreatic Cancer Treatment in India: Ravi’s Inspirational Journey
Pancreatic cancer, though relatively less common, poses a significant health challenge globally. In India, it ranks as the 12th most commonly occurring cancer in men and the 11th in women according to WCRF (World Cancer Research Fund International). However, with advancements in medical science and technology, the outlook for pancreatic cancer patients is improving.
Meet Ravi Kumar, a 45-year-old entrepreneur from bustling Mumbai, India. Ravi’s zest for life and devotion to his family is matched only by his love for diverse cuisines. Two years ago, Ravi’s life took an unexpected turn. He started experiencing persistent abdominal pain, a discomfort he had never felt before. Initially attributing it to a passing ailment, Ravi consulted his local physician, who prescribed some medication. However, the pain persisted and began affecting his appetite.
Concerned, Ravi’s wife, Meera, encouraged him to seek a second opinion. They visited a seasoned gastroenterologist who recommended imaging tests. The results revealed a lesion on Ravi’s pancreas, leading to a biopsy. The diagnosis was pancreatic cancer, a revelation that shook Ravi and Meera to the core.
Determined to find the best care, Meera embarked on extensive research. Her quest led her to MedicoExperts, a prominent name in medical facilitation. With a focus on a comprehensive approach to treatment, MedicoExperts offered Meera an online video consultation with an eminent oncologist, providing her with clarity and confidence in their path forward.
Ravi and Meera decided to travel to India’s capital, Delhi, for Ravi’s treatment. Upon arriving at the hospital, they were met with a sense of reassurance. The hospital’s state-of-the-art facilities and experienced medical staff instilled confidence in them.
Ravi’s treatment journey began with weekly chemotherapy, followed by radiation therapy. When he was deemed ready, a surgical oncologist performed a Whipple procedure, removing a portion of his pancreas and small intestine. The treatment was rigorous, but Ravi’s determination never wavered.
After months of perseverance, the re-evaluation tests brought astounding news – no cancer was detected. Ravi and Meera were overjoyed with the results, attributing their success to the dedicated healthcare team and their decision to seek treatment in India.
Ravi’s story is emblematic of the tremendous progress made in pancreatic cancer treatment in India. With a combination of cutting-edge medical techniques, experienced healthcare professionals, and unwavering patient determination, victory over this formidable foe is possible.
If you or a loved one are facing a similar battle, remember that there is hope and help available. Together, we can conquer even the most challenging circumstances. Choose the best for your health; choose the leading pancreatic cancer treatment in India.
Our Location
We have administrative and consultation offices located in major cities across India, including Mumbai and Delhi.
Best Cancer Hospitals and Treatment – Comprehensive Information
When it comes to cancer treatment, the choice of hospital can make a significant difference in patient outcomes. India has rapidly become a global hub for advanced cancer care, offering a combination of cutting-edge technology, world-class medical expertise, and affordable treatment options. Below is a detailed guide to some of the best cancer hospitals in India, along with an overview of the cancer treatments available.
Why Choose India for Cancer Treatment?
India’s cancer hospitals offer a blend of modern medical infrastructure, highly skilled oncologists, and affordable treatment plans. Patients from across the globe travel to India for cancer care due to the high success rates, availability of advanced technologies like robotic surgery, proton therapy, and personalized treatment plans. Learn more about why India is a top choice for cancer treatment.
Best Cancer Hospitals in India
If you’re searching for the Best Cancer Hospitals in India, you’re in the right place. India is home to some of the leading oncology hospitals in India, offering cutting-edge cancer treatments. These top cancer treatment centers in India are known for their advanced technologies and world-class care. Learn more about the best cancer hospitals in India for detailed information.
Best Oncologists in India
India has some of the best oncologists in India with expertise across different types of cancer. When you’re looking for the top cancer specialists in India, you can rely on these leading cancer doctors in India to provide the best possible care. Visit the best oncologists in India page to find more about the top cancer specialists in India and their qualifications.
Best Cancer Treatments in India
India offers a wide variety of cancer treatments including surgery, chemotherapy, radiation therapy, and immunotherapy. Hospitals are equipped with modern technologies such as CyberKnife, TrueBeam, and Da Vinci Surgical Systems. Learn more about the advanced cancer treatments in India available at top hospitals.
Best Liver Cancer Treatment in India
Looking for the best liver cancer treatment in India? India offers top-tier medical facilities, and some of the best liver cancer hospitals in India are known for their high success rates and innovative treatments. Visit the best liver cancer treatment in India to explore options at advanced liver cancer care in India.
Best Oral Cancer Treatment in India
When searching for the best oral cancer treatment in India, it’s important to choose a facility with a proven track record. The top oral cancer hospitals in India offer world-class care and innovative treatments. Learn more about the best oral cancer specialists in India who are experts in treating all stages of oral cancer.
Best Breast Cancer Treatment in India
For the best breast cancer treatment in India, look no further than India’s top oncology hospitals. These facilities offer the leading breast cancer specialists in India and the most advanced treatment options. Discover more about the top breast cancer hospitals in India where patients receive comprehensive care.
Best Pancreatic Cancer Treatment in India
The best pancreatic cancer treatment in India is available at India’s top cancer centers. These hospitals provide state-of-the-art treatments for pancreatic cancer. Visit the top pancreatic cancer hospitals in India to learn more about the care offered by the best pancreatic cancer specialists in India.
Best Stomach Cancer Treatment in India
If you’re looking for the best stomach cancer treatment in India, the top hospitals in the country offer cutting-edge treatments. Learn more about the top stomach cancer specialists in India and discover the facilities offering leading stomach cancer care in India.
Best Colon Cancer Treatment in India
For the best colon cancer treatment in India, India’s leading hospitals provide top-quality care. Visit the top colon cancer hospitals in India and explore the treatment options offered by the best colon cancer specialists in India.
Best Prostate Cancer Treatment in India
If you’re seeking the best prostate cancer treatment in India, several top hospitals offer advanced care. Visit the leading prostate cancer specialists in India to learn more about the most effective treatments. These top prostate cancer hospitals in India provide innovative solutions for prostate cancer care.
Best Lung Cancer Treatment in India
India is home to some of the best lung cancer treatment centers offering comprehensive care. The top lung cancer hospitals in India provide cutting-edge therapies for lung cancer patients. Learn more about the best lung cancer specialists in India for detailed information on available treatments.
Best Cervical Cancer Treatment in India
Finding the best cervical cancer treatment in India is crucial for successful recovery. The top cervical cancer hospitals in India offer advanced treatment options and world-class care. Visit the best cervical cancer specialists in India to explore more.
Best Bone Cancer Treatment in India
The best bone cancer treatment in India is provided by some of the nation’s top hospitals. Learn more about the leading bone cancer specialists in India and the facilities offering top bone cancer care in India to ensure the best possible treatment outcomes.
Holistic Cancer Care in India
India’s top cancer hospitals not only focus on clinical treatments but also offer holistic care, including nutrition, mental health support, and rehabilitation services. Learn about the holistic cancer care in India provided by leading hospitals to support recovery.
Global Patients and Medical Tourism for Cancer Treatment
India has seen a surge in global patients seeking cancer treatment due to its affordable pricing, high-quality care, and no waitlist policies. The medical tourism for cancer treatment is well-established, with top hospitals offering personalized services for international patients, including accommodation, visa assistance, and follow-up care.